
Primitive Reflexes and Their Role in Chronic Pain and Muscle Tension Issues
The Empowering Knowledge and Practical Solutions of Dr Joaquin Farias

Introduction
Avid readers will have noted I’ve mentioned the work of Dr Joaquin Farias a few times in my articles. Indeed, in my recent article,

I noted that his ground breaking “cortical shock” theory is one of the central pillars of my own thinking on understanding human suffering. Here, we will take a deeper dive into Dr Farias’s discoveries and explore how and what this informs us about healing.
Dr Farias is a (the?) world expert in dystonias, which manifest as often painful muscle contractions, tics, spasms and tremors. Dystonia can occur in a variety of chronic illnesses, traumas, neurological, and movement issues, and so Dr Farias’s work is directly relevant to conditions such as Parkinson’s Disease (generalized dystonia), Fibromyalgia, MS, Stroke, Chronic Pain, Restless Leg Syndrome, and so forth.
Dr Farias’s Journey of Discovery
I think it is useful for us to first go on the journey that Dr Farias himself went through in helping hundreds and thousands of people with various forms of dystonias, as he describes it in his seminal book "Limitless. How Your Movements Can Heal Your Brain: An Essay On The Neurodynamics Of Dystonia". Here, Dr Farias explains how he realized some truly amazing, and profoundly important, things.
“These patients sent me videos so I could analyze their movements, and I sent them my opinion. In a very short time, I had accumulated videos of thousands of patients, which allowed me to go on to the next level of my research. “
“I decided to look for a pattern that would explain every one of those cases. To do this, I gathered photos of positions from every video and classified them by categories... To my surprise, there weren’t that many categories. It seemed that there were some muscles that were dystonic and others that never were. I classified hypertonic (greater tension than the expected) and those that were hypotonic (less tension than the expected) and assigned a number to each level of tension.”
The figure below, adapted from Dr Farias’s book, shows the muscles which can become hypertonic and painful (red dots), and those which can become hypotonic and forgotten (blue dots). One thought that these images triggered in me is that the blue, numbed areas are more or less the parts that are exposed, and hence needed to be desensitized to attacks, when curled up in the fetal or crouching position with arms over the head, and the red areas are the parts that are protected in this position. Hence this indicates to me that these patterns may somehow be connected with defensive Nervous System states against perceived lethal levels of danger.
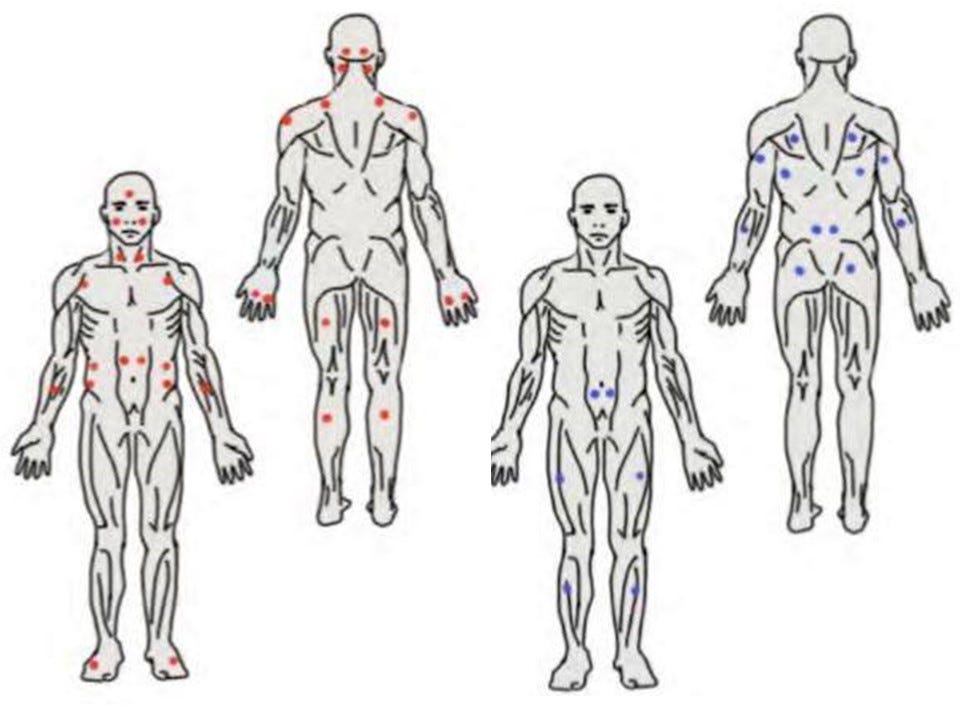
“These hypertonic points corresponded to specific muscles that were not being correctly controlled by the nervous system.”
“This pattern, undescribed until now, shed light on the affected neural circuits which are common in a variety of different pathologies. Considering the great number of muscles present in the human body, the fact that only a limited number of them become dystonic is no less than a great discovery.”
“I believe that these hypotonic areas are the cause of the hypertonic ones. The neural pathways that become silent fail to modulate the movement of the muscles they control, which become hypotonic. The antagonist muscles associated with these hypotonic ones react in a compensatory manner, increasing their hypertonic tension.”
This is one of the profoundly important findings of Dr Farias - that the hypertonic and painful parts are the effect and not the cause, and the real issues stems for the silenced neural pathways to the forgotten flaccid muscles!
Dr Farias goes onto to explain how different combinations of tension points result in certain positions and postures in the people he helps.
“A pattern of position combinations began to appear – and I finally understood. If I looked at all the postures of the thousands of people with dystonias, and put them together, suddenly it all made sense."
He noted that all the positions had a use, such as grabbing objects, the movements made by the eyeballs to avoid bright light when blinking was not enough, biting, breathing, etc. He found that combing the positions of multiple patients, just a few overall patterns emerged.
What Dr Farias noticed was these overall patterns were very familiar, and will be familiar to parents everywhere. They were all the positions that babies regularly adopt!
Primitive Reflexes
According to the wikipedia article:
“Primitive reflexes are reflex actions of the Nervous System that are exhibited by normal infants, but not neurologically intact adults, in response to stimuli. These reflexes are suppressed by the development of the frontal lobes as a child transitions normally into child development. These primitive reflexes are also called infantile, infant or newborn reflexes.”
Note the very direct linkage made between “suppressed by the (pre)-frontal lobes” and as children develop normally. This will be very important later.
There are many of these reflexes, which include the automatic closing of fingers if the palm is touched, the curling of the toes when the sole of the foot is touched, the turning of the neck, etc. Here are a few very quick videos showing some examples. You can find many more videos on youtube.
According to Dr Farias’s book, Primitive Reflexes are involuntary responses to tactile, proprioceptive [senses of where body parts are and what they are doing], or vestibular [sense of balance] signals. These are evolutionary responses which are innate and not learned. These reflexes consist of movements which are automatic, are “pure, essential, logical and effective responses” that allow newborns to “meet complex challenges such as protecting themselves, passing through the birth canal, changing positions, finding food, breathing or moving around”. They are usually associated with feeding, breathing, fight, flight, or freeze responses.
A baby is supposed to leave those reflexes behind when other, better, voluntarily or controlled responses are learned during development, and should wane by about the age of four to six months. The control occurs at a frontal or prefrontal cortex level (hint, hint: remember we mentioned Dr Farias ‘cortical shock’ theory in the introduction). So, as we develop, the pre-frontal cortex learns voluntary control of movements, which can override or inhibit these Primitive Reflexes of the brain stem. Some involuntary reflexes do continue through life, such as blinking reflex, coughing, gagging, sneezing, yawning, etc., but most are supposed to get integrated in infancy.
The key important point here is that these Primitive Reflexes do not disappear or go away, they are merely suppressed or inhibited due to the development of the frontal cortex.
Many developmental issues in children are linked to one or more of these Primitive Reflexes not being correctly inhibited or integrated in early life. See, for example, Rhythmic Movement Training methods which can help with physiological, psychological, and behavioural problems in children by helping to integrate the Primitive Reflexes properly and in the correct order.
The Cortical Shock Theory and Primitive Reflex Re-emergence
Armed with the above background material, we can now complete the circle, and see what the big picture that Dr Farias’s work reveals. Recall that Dr Farias’s theory of chronic conditions involves a ‘cortical shock’, whereby a stressful episode causes the cortex of the right brain hemisphere to go into hibernation and shutdown, and that, according to Bonnie Badenoch’s work, this can also happen due to trauma.
As we have seen, the pre-frontal cortex is the very area of the brain which is responsible for inhibiting the involuntary Primitive Reflexes controlled by the brain-stem. So what happens when the right hemisphere goes into shock/shutdown? It can no longer suppress or control the Primitive Reflexes properly, and hence some of these may partially or fully re-appear or re-emerge in our adult lives, but in a dysregulated way!
I believe it is worth anyone with chronic pain, muscle tensions, Nervous System dysregulation, or movement disorders looking into at and pondering all the different types of Primitive Reflexes, and view them in action, e.g. as in the videos of babies above. I am almost certain that you will find that a maladaptive re-emergence of one more reflex will explain many of your symptoms.
TMJ or jaw pain? Probably the re-emergence of the biting or suckling reflex! Painful toe curling and plantar fasciitis? Likely the re-emergence of the plantar or Babinksi reflex! Neck pain? Maybe the asymmetric tonic reflex in action, … and so forth.
Once we educate ourselves about Primitive Reflexes, we see that Dr Farias is spot on, and we can realize that many physical "symptoms" are actually just the semi-permanent activation of one or more maladapted, re-emergent reflexes. Indeed, specific re-emergent Primitive Reflexes are actually already used as key diagnostic points in chronic conditions, such as the Glabellar Reflex in diagnosing Parkinson's Disease. Hence the link between these and various neurological and Nervous System disorders are well established.
An important point here is to see and understand the Primitive Reflexes as survival driven and vital, and that it is not these which are really the problem. They only come back when the pre-frontal lobes of the right cortex goes into a shock state and hence can no longer do the job of inhibiting these built in survival reflexes. Remember that right hemisphere cortical shocks mainly arise through trauma, chronic stress and exhaustion, and it these which are the actual fundamental causal issues at play. The Primitive Reflexes, chronic pain, and muscle issues are all downstream of this.
Returning now to those hypertonic and hypotonic muscles to complete the picture, a key point of Dr Farias's work is that the real underlying muscular problems are in those specific muscles which would normally prevent the Primitive Reflexes from activating, and that these are “forgotten” when the pre-frontal cortex goes into shock. It is the neural pathways of the brain activating and sensing these muscles getting switched off during the cortical shock, which causes the reflexes to re-emerge. These muscles are not the tense ones, but the ones that become weak and flaccid (hypotonic).
Other muscles then became overactivated, tense and rigid and painful in an attempt to overcompensate for the forgotten ones, these muscles become "hypertonic". While most therapies will target the hypertonic, painful muscles, Dr Farias says:
“look after the hypotonic ones, and the hypertonic ones will look after themselves.”
Pragmatics: What to Do?
The very good news is this can all be rectified by taking relevant action, and employing the empowering knowledge that Dr Farias has given us. The re-emergent can be re-absorbed, in a similar process to how this was achieved the first time around.
The first thing we need to do is to address the chronic stress, trauma, and exhaustion that is causing our pre-frontal cortex to shut down in the first place. This involves introspection, taking stock of our lives, and our behaviours, and making all the necessary changes we can, including prioritizing rest, relaxation and sleep, to bring us of out of cortical shock. I keep a master of list of suggestions of things which can help in my first substack article:
Next, we need to reconnect those hypotonic muscles with the brain again, and re-learn how to inhibit the problematic Primitive Reflexes.
“In order to walk once again, or use the hands again, or see again, [people] needed to return once again to do what they did as infants in order to overcome the primitive responses and substitute them for more evolved ones.”
In other words, we need to re-start the process that we went through in learning how to move as infants again, but this time armed with the full knowledge of how we achieved it, so re-learning the right moves in the right order, and taking this process one “baby step” at a time, will be key.
Dr Farias’s techniques are hence movement based therapies, optimally designed to achieve this re-integration. That his methods can work dramatically for some people is highlighted by a famous video, where he gets a wheelchair bound former ballerina with generalized dystonia up and dancing again in short order.
Based on these understandings, vast knowledge, and unrivalled experience of helping folks with dystonias, Dr Farias has also developed an online Dystonia Recovery Program, which is well worth exploring, much of which I have integrated into my own personal recovery.
For myself, as I mentioned in my previous substack article,
I found two modalities which have fast tracked my symptom reduction. I believe these work by reconnecting the brain and the body, and by also removing the mental/psychic blocks of the stressful episodes (body memories) that caused the disinhibition of the Primitive Reflexes in the first place: Deanna Hansen's self-care fascia decompression modality Block Therapy, which works through the body, and Lilian Sjøberg's HOPE-shortcut talking therapy, which works through the mind, to release body memories of stressful events. These two modalities combined have allowed me significant progressive symptom reduction, especially in regards to pain and dystonia in my right neck and shoulder.
Wonderful article! I met with Dr Farris in November of 2015 and I did his exercises as directed. By February my dystonia had abated and my balance was so improved that it was doubtful that I had PD.
Fascinating. Thank you for boosting this knowledge, Gary.